Bladder cancer usually affects older people, with a sharp increase in incidence after the age of 55. These patients are often smokers and usually have a number of medical problems (including heart disease, diabetes and high blood pressure). This means that when surgery is necessary, these patients are at higher risk of complications.
In aggressive bladder cancer, the recommended treatment is usually cystectomy, which involves the removal of the entire bladder. Once the bladder is removed, urinary diversion must be performed, which means the creation of an alternative way to bring urine out of the body. This is most often achieved via one of two methods:
- ileal conduit/urostomy (see Figure 1): a piece of small intestine is used to create a tube (conduit). The remaining urinary tract is connected to the conduit. Urine drains into the conduit and passes outside the body through a hole in the wall of the abdomen (stoma) and fills a bag that is attached to the skin. The bag needs to be drained periodically and regularly replaced.
- neobladder (see Figure 2): a longer loop of small intestine is used and reshaped into a bladder. It is placed in the same location as the original bladder, and one end is joined to the remaining urinary tract, and the other end is joined to the urethra. In these cases, patients can eventually still pass urine from their urethra.
Traditionally, cystectomy has been done with the open technique, where a 15-20 cm long incision is made in the lower part of the abdomen for the surgery. However, complications after open cystectomy are common, with more than 50% of patients experiencing complications after surgery, and around 30% are readmitted after discharge.
Even with the introduction of the surgical robot for ‘key-hole’ cystectomy, many surgeons were using a hybrid approach. In these cases, removal of the bladder was done with the robot, but a separate 10-15 cm long incision was made to create the urinary diversion (extracorporeal urinary diversion). Essentially the urinary diversion in these surgeries were done by the open method, due to the technical challenges with handling and suturing the small intestines with the robot. Unfortunately, a number of studies have shown limited benefits for this hybrid type of robotic cystectomy, compared to traditional open surgery.
About two months ago, a large study was reported from the United Kingdom, where a total of 338 patients with bladder cancer were randomized to receive robotic cystectomy with intracorporeal urinary diversion, or open surgery. In robotic cystectomy with intracorporeal urinary diversion, the entire surgery, including urinary diversion, is performed in a ‘key-hole’ manner with the robot. Unlike extracorporeal or hybrid robotic cystectomy, there is no need to make a separate 10-15 cm long incision for the surgery. This is technically demanding and the trial only allowed experienced robotic surgeons who had completed at least 30 cystectomies as the sole operator to perform the cases. This study reported a number of key advantages for a totally robotic approach for cystectomy. These include:
- Reduced time in hospital. This included the hospital stay after surgery, and readmissions after discharge from hospital.
- Less wound complications, and less thromboembolic complications after robotic surgery. This is likely due to the smaller incisions for robotic surgery, with resultant reduction in pain allowing patients to get out of bed earlier after their operation. This will reduce the chances of getting a thromboembolism after major surgery.
- Better quality of life. Patients had to answer questionnaires as part of this study. At 5 weeks and 12 weeks after surgery, patients who underwent robotic surgery reported significantly higher health-related quality of life.
- Lower disability. Patients had to answer questionnaires as part of this study. Significantly more disability was reported in the open surgery patients compared to the robotic surgery group at 5 weeks and 12 weeks after surgery.
- The ‘cure’ rates were similar, with no difference in cancer recurrence rates with either approach.
Aggressive bladder cancer can be a deadly disease. However, there is now strong evidence that with a totally robotic approach, cystectomy performed by experienced robotic surgeons can lead to improved outcomes and faster recovery in these patients. In conclusion, for patients who have bladder cancer, talk to your urologist about surgery techniques available, and whether robotic cystectomy with intracorporeal urinary diversion is possible.

Figure 1. Ileal conduit / urostomy
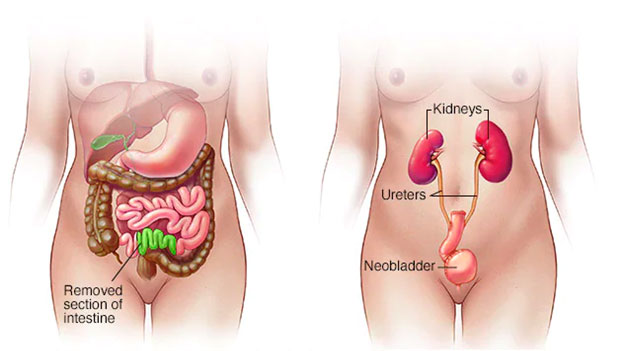
Figure 2. Neobladder
Reference:
Catto JWF, Khetrapal P, Ricciardi F, et al. Effect of Robot-Assisted Radical Cystectomy With Intracorporeal Urinary Diversion vs Open Radical Cystectomy on 90-Day Morbidity and Mortality Among Patients With Bladder Cancer: A Randomized Clinical Trial. JAMA. 2022;327(21):2092–2103. doi:10.1001/jama.2022.7393
Catto JWF, Khetrapal P, Ricciardi F, et al. Effect of Robot-Assisted Radical Cystectomy With Intracorporeal Urinary Diversion vs Open Radical Cystectomy on 90-Day Morbidity and Mortality Among Patients With Bladder Cancer: A Randomized Clinical Trial. JAMA. 2022;327(21):2092–2103. doi:10.1001/jama.2022.7393