WHAT IS PROSTATE CANCER?
Prostate cancer is the cancer of the prostate gland. The prostate is a walnut-sized gland in between the bladder and the urethra that produces the fluid that nourishes and transports sperm. Prostate cancer is the second most common cancer among men in Singapore.
SYMPTOMS OF PROSTATE CANCER
Early-stage prostate cancer has few or no symptoms as the cancer develops relatively slowly. If symptoms appear, they may include difficulty in passing urine, burning sensation while urinating, blood in urine, loss of appetite and/or weight, and lower back pain.
DIAGNOSING PROSTATE CANCER
Men with either abnormal Prostate Specific Antigen (PSA) blood test and/ or abnormal digital rectal examination of the prostate are considered at higher risk of having prostate cancer. However, prostate cancer can only be diagnosed through a biopsy. A Magnetic Resonance Imaging (MRI) scan of the prostate is usually performed before the biopsy to visualize areas within the prostate that are suspicious for harbouring prostate cancer.

MAGNETIC RESONANCE IMAGING (MRI) TARGETED BIOPSY OF THE PROSTATE
Elevated levels of PSA can be associated with a number of reasons. These include infection, prostatic enlargement but most concerning of them all, prostate cancer.
In the past, to exclude prostate cancer in patients with raised PSA, the patient would be subjected to a systematic or random biopsy of the prostate. This involves 12 biopsies taken from the prostate in a random manner. As such, it is possible to miss a cancer, and in the event that the biopsy was negative for cancer, the patient would have to undergo another random biopsy if the PSA was still elevated.
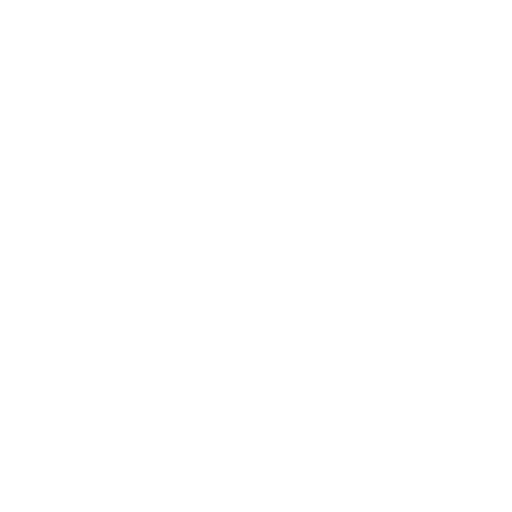
In recent years, we have discovered that MRI of the prostate can offer valuable insights as to whether an elevated PSA is due to cancer. As such, using MRI and fusion with ultrasound, we can now do targeted biopsies of the prostate. This allows for a quantum leap in accuracy of the biopsies and reduces the need to repeat them. This also lowers the risk of infection with repeated biopsies. Targeted biopsy of the prostate can be carried out under sedation or local anaesthesia and patients usually can be discharged on the same day.
At Urohealth Medical Clinic, we offer MRI Targeted Biopsy of the prostate. Dr Tan Yung Khan, Medical Director and Senior Consultant Urologist of Urohealth Medical Clinic, established MRI Targeted Fusion Biopsies of the Prostate using the UroNav Platform in Asia.
TRANSPERINEAL OR TRANSRECTAL BIOPSY OF THE PROSTATE
As the prostate lies just in front of the rectum, traditionally, prostate biopsies have been performed by passing the biopsy needles through the rectum into the prostate. This is known as a Transrectal Prostate Biopsy. Unfortunately, the rectum is full of bacteria and studies have reported that the risk of severe infection (sepsis) after prostate biopsies can range between 2 to 10%! To mitigate the risks of infection, doctors have tried various measures including giving stronger or multiple antibiotics, or tailoring the antibiotics based on the bacteria grown from a swab of the rectum. However, all these techniques have not managed to eliminate the risk of sepsis, and antibiotics themselves can lead to complications including diarrhoea and other digestive issues, allergic reactions and promoting antibiotic resistance.
An alternative approach is the Transperineal Biopsy. In this biopsy technique, the biopsy needle is passed through the skin behind the testicles (known as the perineum), and do not pass through the rectum. As skin can be easily cleansed compared to the rectum, the risk of sepsis after a Transperineal Prostate Biopsy is near zero, with data showing a risk of sepsis of less than 0.1%. In fact, in Europe, it is the recommended technique for prostate biopsy (as per the European Association of Urology practice guidelines) ahead of the traditional biopsy through the rectum. Dr Tan Teck Wei, senior consultant urologist at Urohealth Medical Clinic, introduced Transperineal Biopsy under local anaesthesia in the region. With good local anaesthesia nerve blocks (and sometimes with light sedation), the entire biopsy can be done in the clinic, usually through two tiny punctures in the skin of the perineum.
WHY DO IT WITH US?
Both Dr Tan Yung Khan and Dr Tan Teck Wei routinely perform MRI Targeted Fusion Transperineal Prostate Biopsies.
Dr Tan Yung Khan established the MRI Targeted Fusion Biopsies of the Prostate using the UroNav platform in Asia. In his published series, he has shown that in his hands, there has been a significant improvement in the detection of clinically significant prostate cancer. Dr Tan Yung Khan has also gone on to set up the Asia Pacific Centre of Excellence for UroNav guided targeted biopsies and has given talks and run masterclasses for urologists in the region on the use of this system.

Dr Tan Teck Wei established the Transperineal Prostate Biopsy technique in Southeast Asia and published the first report on Transperineal Prostate Biopsy under local anaesthesia in a clinic setting in the region. In his series, there have been no cases of urinary infection or sepsis after this biopsy. The technique is safe, effective, and well tolerated.

TREATMENTS FOR PROSTATE CANCER
Treatment will depend on the stage of the cancer, and is also influenced by the aggressiveness of the disease. Prostate cancer is divided into whether it is localised to the prostate, or if it has spread to other organs or parts of the body (metastasis).
LOCALIZED PROSTATE CANCER
ACTIVE SURVEILLANCE
For low-grade (i.e., low aggressiveness) localized prostate cancer, active surveillance is an option due to the low risk of cancer growth and spread. However, patients are required to visit their urologists regularly for blood tests, rectal examinations and periodic repeat MRI scans and prostate biopsies. All these measures allow their urologist to detect changes in the cancer and recommend treatment if and when appropriate. For patients unwilling to undergo active surveillance, alternatives include surgery or radiation therapy.
For higher grade localized prostate cancer, the standard treatments are surgery or radiation therapy. A new type of treatment, called focal therapy, has generated a lot of interest but is still considered investigational.
SURGERY (ROBOTIC RADICAL PROSTATECTOMY)
Surgery involves removing the prostate and the surrounding tissues completely. This includes removal of the surrounding lymph nodes, especially for high-grade cancers. The gold standard surgical option nowadays is:
ROBOTIC RADICAL PROSTATECTOMY
- Compared to conventional open surgery, Robotic Radical Prostatectomy is less traumatic and minimally invasive. Using the robot also improves the surgeon’s visualization, dexterity and precision compared with open or laparoscopic surgery, while enabling the entire operation to be done through six small incisions around 1cm in size.
- Two of the main long-term side effects of surgery are erectile dysfunction (inability to achieve or sustain erections for sexual intercourse) and urinary incontinence (involuntary leakage of urine, requiring patients to wear pads or diapers).
- Nerve-Sparing Robotic Radical Prostatectomy: The nerves that help control erections lie closely on each side of the prostate. Patients who are sexually active, and who do not have extensive or aggressive prostate cancer, are suitable for Nerve-Sparing Robotic Radical Prostatectomy. With the improved visualization and precision of the robot, these nerves can be meticulously freed away from the prostate during the surgery. With nerve-sparing prostatectomy, up to 50-75% of patients may be able to achieve erections sufficient for sexual intercourse after surgery.
- Retzius-Sparing Robotic Radical Prostatectomy: This is a technically challenging modification of the conventional Robotic Radical Prostatectomy, but has been proven to improve early return of urinary continence after surgery. The space of Retzius is an area behind the pubic bone and in front of the bladder and prostate. This area contains the strong ligaments and structures that anchor and support the prostate and bladder, which are crucial in the maintenance of continence in men. In conventional Robotic Radical Prostatectomy, the space of Retzius is opened up and these ligaments and structures are cut in order to gain access to remove the prostate. In Retzius-Sparing Robotic Radical Prostatectomy, the prostate is approached from behind through a small incision in the peritoneal lining between the bladder and colon. The space of Retzius is undisturbed during the surgery. Dr Tan Teck Wei and Dr Tan Yung Khan are among a handful of surgeons in Asia who can offer this surgical technique to appropriate patients.
RADIATION THERAPY
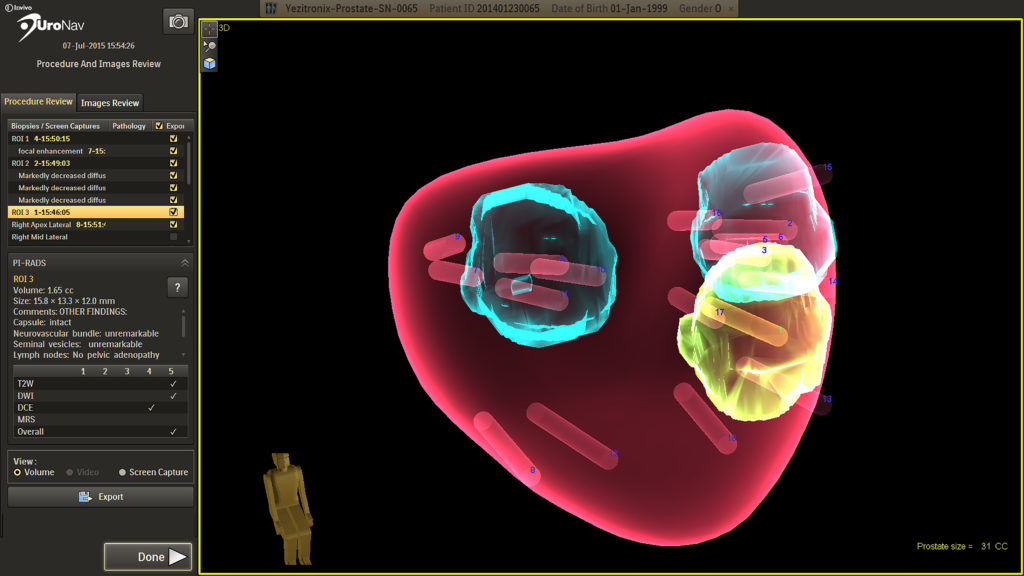
Radiation therapy involves utilising high doses of radiation to kill prostate cancer cells. At low doses, radiation is used in x-rays to see inside your body, such as x-rays of the chest or bones. The most commonly used type of radiation therapy for prostate cancer is called external beam radiation therapy (EBRT), in which a machine aims radiation at the cancer from outside the body. It is considered as effective as surgery for the treatment of localised prostate cancer and is the standard alternative in all the prostate cancer treatment guidelines.
Potential downsides to radiation therapy include:
- Longer treatment duration: Patients usually have to go for daily radiation therapy sessions for between 4 to 8 weeks before the treatment is completed.
- Treatment is often combined with androgen deprivation therapy: Patients are usually given injections that block testosterone production for between 6 months to 3 years. When men do not have testosterone, side effects can include hot flashes, loss of interest in sex, erectile dysfunction, loss of muscle mass and physical strength, and loss of bone density.
- Risk of damage to surrounding organs: although radiation therapy is focused on the prostate, there is a very small risk of damage to the bladder or rectum, which is adjacent to the prostate. If this occurs, side effects can include blood in the urine or stools, and urinary urgency and leakage. In addition, there is an approximately 1% risk of secondary cancer developing in the bladder or rectum in the long term. There is also a risk of erectile dysfunction after radiation therapy.
Proton beam therapy has recently gained a lot of attention as an attractive alternative to conventional EBRT, with promises of lower side effects to the adjacent organs. However, there is still lack of evidence that proton beam therapy has an advantage over conventional radiation therapy, and according to prostate cancer treatment guidelines, it can only be regarded as an experimental alternative treatment.
FOCAL THERAPY
Surgery or radiation therapy, which have been mentioned above, are known as whole gland treatment as the entire prostate is removed or irradiated. As a result, these treatments can potentially result in urine incontinence and erectile dysfunction in some patients. The reason is that the nerves, blood vessels, and muscles that determine urine control and erection are in close proximity to the prostate gland and are thus often damaged in whole gland treatments.
With the advent of more accurate MRI-targeted prostate biopsies in the last few years, some patients are diagnosed with cancer only involving a small proportion of the prostate. In these men, the logical thought is whether treatment can be focused only on these areas of cancer without needing whole gland treatment. This is also known as focal therapy as only the region of the prostate where the cancer is located is treated. This approach can potentially improve the functional outcomes of treatment (i.e., lower the risk of urine incontinence and erectile dysfunction) without sacrificing control of the cancer that is achieved with whole gland treatment.
There are many energy sources that have been used for focal therapy, but the two most common types reported in studies are high-intensity focused ultrasound (HIFU) and cryotherapy. In HIFU, heat is generated by an ultrasound probe placed in the rectum and directed towards the region with prostate cancer, resulting in death of the cancer cells. For cryotherapy, probes are placed through the perineal skin into the area of prostate cancer, resulting in freezing and death of the cancer cells.
Focal therapy is a newer approach to treating prostate cancer, and as such, studies have follow up of up to 10 years after treatment. Most of these studies find that approximately 20-30% of prostate cancer can persist or recur after focal therapy. These areas of cancer may then either require repeat focal therapy or whole gland treatment. In terms of functional outcomes after focal therapy, studies have confirmed excellent outcomes, with continence rates of over 97% and preserved erection function in more than 75% of patients.
Although the data for HIFU and cryotherapy for focal therapy of prostate cancer is building up, it is currently still not considered standard of care in international guidelines. It is recommended that the data of patients undergoing HIFU or cryotherapy is tracked and analysed to provide more evidence of the effectiveness of focal therapy. At the moment, based on expert consensus, the ideal patient for focal therapy is someone with a small area of Gleason grade group 2 to 3 cancer, who has undergone an accurate MRI-targeted and systematic biopsy to exclude aggressive cancer outside the proposed area for focal therapy. Dr Tan Teck Wei and Dr Tan Yung Khan are able to offer focal cryotherapy for suitable prostate cancer patients.
METASTATIC PROSTATE CANCER
For cancer that has spread outside the prostate, although there is no cure for the cancer, it can be controlled effectively with treatment. With the introduction of multiple types of treatment options in the last few years, survival for metastatic prostate cancer has improved dramatically. Some of these treatments include:
- Androgen deprivation therapy: The main driver of prostate cancer growth is the male hormone testosterone. In androgen deprivation therapy, usually injections are given to block the production of testosterone by the testicles. This will help to shrink and retard the growth of prostate cancer cells. An alternative is surgical removal of the testicles (also known as orchidectomy).
- Novel hormonal therapy: Oral medications are given, which act differently from the usual androgen deprivation therapy. These medications block the androgen receptor on the prostate cancer cells, further blunting the ability of testosterone to fuel cancer growth.
- Chemotherapy: intravenous drugs are given to destroy the cancer cells.